Marvellous Medical Material of the Moment: Soap
05 June 2017

Soaps - and their newer synthetic cousin detergents - are substances that play an important role in cleaning by removing dirt and grease from our bodies and lived environment. Although there are many different recipes for soap, the basic chemistry involves boiling an oil or fat with an alkali. The ensuing reaction, called ‘saponification’, produces soap and glycerine.
Historically, the fats used for soap production would have been either animal fats like tallow and bone grease or vegetable oils such as olive oil, palm oil or coconut oil. The alkali component, potash or soda, would have been derived from the ashes of plant matter. Developments in the chemistry of cleaning agents have since led to the production of a plethora of different kinds of soap: from beauty soaps to antibacterial and medicated soaps. Non-soap synthetic detergents were also introduced after WWII following a shortage of animal and vegetable fats and in response to the need for cleansing agents that would work in mineral-rich and cold water.
Both soaps and detergents work to remove ‘soils’: the combination of bacteria, moulds, yeasts, fats, grease, proteins and minerals that build up on surfaces and our skin. Soils are often hard to remove from surfaces because they are hydrophobic and repel water molecules. At the same time, the surface tension of water (the strong attraction of water molecules to each other) causes it to bead and stops it properly wetting or saturating a surface. Soaps and detergents are surfactants: compounds that reduce the surface tension of water, allowing it to flow more freely over a surface. Their molecules also contain both hydrophobic and hydrophilic components that attach to the oil and water respectively and form a bridge between them. This allows the oil and dirt to mix with and become suspended in the water as an emulsion that can then be removed.
Today we mainly associate soap with cleanliness and health, and in particular with personal hygiene. However, early forms of soap were used for everything except cleaning the body. The earliest evidence of soap-making can be found in ancient Sumerian and Babylonian texts that date back to the 3rd century BC. The Phoenicians, Gauls and Romans also made saponaceous substances, but these were largely used in the preparation of wool for dying or for bleaching and styling hair: not for personal hygiene. Naturally occurring ‘soapweeds’, clays, perfumed oils and mechanical cleaning implements were used to clean the body instead (Levey 1954; Bradley 2002).
It is still debated exactly when soap was first used for personal hygiene and prevention of disease, with some arguing that the Greek physician Galen discussed its medicinal and body-purifying benefits as far back as the 2nd century AD (Partington 1960). The manufacture and use of soap grew slowly in Europe from the 7th until the 18th centuries, existing as localised and small scale craft production centred around cities like Malaga and Alicante in Spain, Genoa and Venice in Italy, Marseilles in France and Bristol, Coventry and London in England. The period between the late 18th and 19th centuries saw a series of significant advances in chemical knowledge that led to the birth of the modern soap-making industry, including the development of inexpensive synthetic caustic soda (Gibbs 1939). These technical developments allowed soap-making to move from a small-scale craft to an industry.
But it was the late 19th century that saw a massive and rapid expansion in soap production and sales, particularly in Britain. The emergence of germ theory – the idea that microbes caused disease - played a very important role in soap’s transition from luxury good to everyday necessity. Against a prevailing idea that infection and disease were caused by ‘miasmas’, vapours or smells coming from stagnant water and waste matter, medics like American physician Oliver Wendell Holmes and Hungarian obstetrician Ignaz Semmelweiss began to put forward the idea that they might be transmitting disease to patients by contact. They instituted handwashing or disinfecting techniques in hospitals that substantially reduced death rates (Tebbe-Grossman and Gardner 2011).
The virtues of handwashing and antisepsis were not immediately widely recognized. Historian of science Steven Schaffer argues that the ‘fight for soap’ required a ‘distinctive late Victorian combination of scientific authority, respectable domesticity and mass advertising’ to succeed (2004). He discusses the role of public lectures and demonstrations of scientists like Huxley and Tyndall in this popularisation of pathologies of infection (2004). Anthropologists Jamie Cross and Alice Street (2009) also cite the importance of marketing strategies like Lifebuoy soap’s campaigns, which emphasised the dangers of invisible germs on door handles, banisters and other people, in creating new consumer subjectivities.
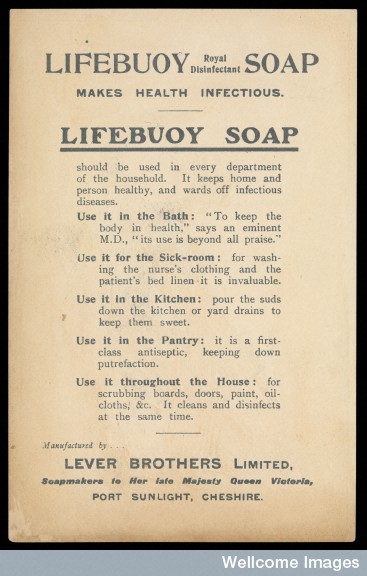
Image credit: Wellcome Library, London.
The widespread availability and increased use of low-cost soap did a lot to improve levels of hygiene in 19th century Britain, and led to many of our contemporary cleaning practices. Soap-like substances had been used medically as purgatives and to treat skin conditions since the Egyptians and Greeks (Gibbs 1939). However, the development of specially made medicated soaps was first taken up in a scientific manner between the 19th and early 20th centuries (Appleton & Simmons 2007). At the advice of surgeons and dermatologists these medicated soaps incorporated ingredients like phenol (carbolic acid), sphagnol (peat tar), glycerine, salicylic acid, formaldehyde or mercury salts that were effective as germicides and for skin conditions like eczema and psoriasis. However, as Steven Connor shows, some of the health claims made for medicinal soaps were ‘large and improbable’, such as the use of Amiral as a topical treatment for obesity (2013). Some medicated soap additives like mercury compounds were also later shown to have serious long-term negative health effects and were banned from soaps and cosmetics in Europe and the US, although they are still found in cosmetics globally.

Photo credit: Adrian Wressell, Heart of England NHSFT. Wellcome Library, London.
The efficacy of different formulations of soaps and detergents continue to be debated by medical professionals and in the public domain. The most well-known example of this is probably the debate surrounding the widespread use of antiseptic agents such as triclosan that are incorporated into soaps and sutures used in hospitals as well as toothpastes and plastics in consumer products (Page et al. 2009). The main concern in the scientific community focuses on the overuse of disinfectants and the role that may play in inducing antimicrobial resistance (McMurray et al. 1998), whereas the media furore, rebuffed by the NHS (2014), focused on triclosan’s potential toxicity (Willey 2014). Laboratory tests and clinical trials have both reinforced and contested concerns around resistance (Aiello et al. 2007), but in the UK clinicians remain in favour of using triclosan in, for example, sutures, where demonstrable health benefits can be shown as opposed to in consumer applications where no benefits have been shown (Leaper at al. 2011).
Wow, what a whistle-stop tour! That’s all for this marvellous medical materials.
For the full list of references see the Material Anxieties project page.